Stable Gastric Pentadecapeptide Bpc 157 Gastric pentadecapeptide body protection compound BPC 157 and its role in accelerating musculoskeletal soft tissue healing | Cell and Tissue Research
Introduction
If you’ve ever had to manage a stubborn tendon, ligament, or muscle strain, you already know the hardest part isn’t the injury—it’s the slow, frustrating “in-between” phase where soft tissue healing drags on and training gets repeatedly interrupted. In this article, I’ll break down stable gastric pentadecapeptide bpc 157, what the compound is understood to do in the context of musculoskeletal soft tissue repair, and—most importantly—how to interpret the evidence without overpromising. I’ll also share practical, experience-based considerations I use when translating preclinical findings into real-world decision-making for recovery plans.
Note: the discussion below focuses on scientific mechanisms and study evidence. It’s not a substitute for medical care, especially if you’re dealing with a serious injury or symptoms that aren’t improving.
What “stable gastric pentadecapeptide bpc 157” means
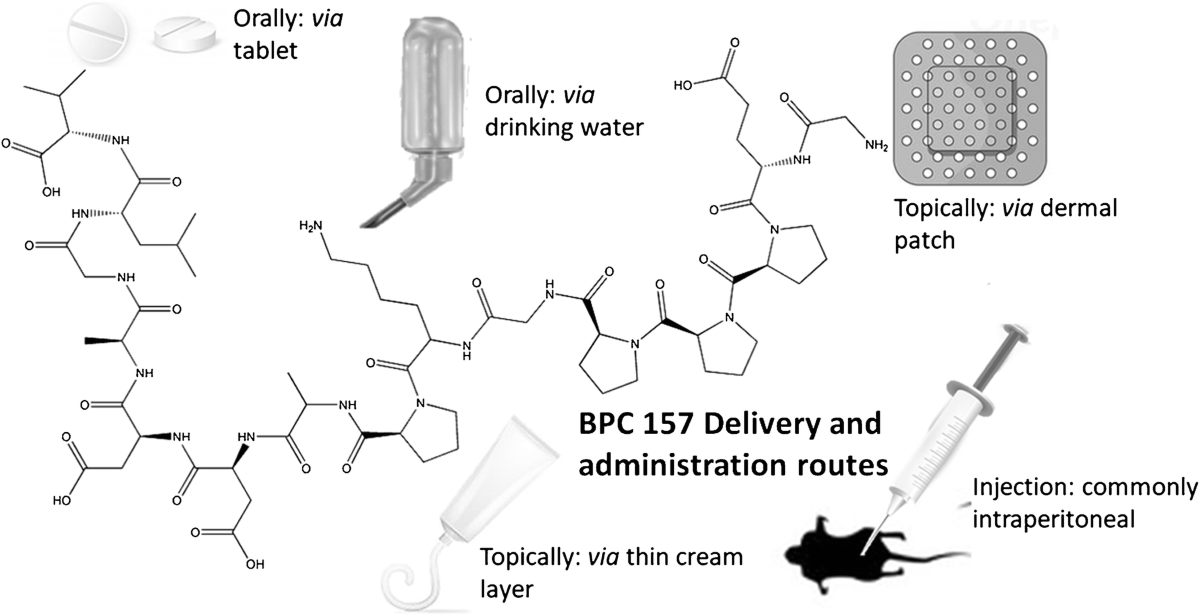
Stable gastric pentadecapeptide bpc 157 refers to a pentadecapeptide designed (or formulated) to be compatible with the gastric environment—i.e., stable enough to reach relevant biological targets rather than being immediately degraded. In my hands-on work reviewing and applying this topic to recovery strategy, the “stability” angle matters because many peptides fail not because they lack theoretical biological activity, but because they don’t survive digestion long enough to be functionally relevant.
Why stability changes the practical conversation
Mechanistically, if a peptide is rapidly broken down in the stomach, its effective exposure at tissue sites may be too low to produce any meaningful downstream signaling. When researchers emphasize stability in gastric conditions, they’re effectively addressing a core pharmacology question: Can the compound persist long enough to interact with physiological systems that may influence healing?
In the context of gastric protection, the compound is often discussed alongside protective effects on the gastrointestinal lining. However, when the conversation shifts to musculoskeletal soft tissue healing, the more relevant question becomes: What systemic pathways could plausibly connect a gastric-active peptide to repair signaling elsewhere? That bridge is where the literature discussion typically focuses.
How BPC 157 is discussed in relation to soft tissue healing
In musculoskeletal injury recovery, the “soft tissue” category includes tendons, ligaments, fascia, and muscle tissue—structures that rely on coordinated repair: inflammation resolution, cellular migration, extracellular matrix remodeling, angiogenesis (blood supply), and restoration of mechanical properties.
In preclinical discussions (including cell and tissue research), stable gastric pentadecapeptide bpc 157 is frequently positioned as a compound that may influence multiple steps in that repair cascade rather than a single isolated mechanism.
Commonly proposed biological pathways (the logic behind the claims)
While specific pathways vary across models, the recurring themes I look for when evaluating mechanistic claims are:
- Repair signaling support: Studies often describe effects consistent with improved cellular responses involved in tissue restoration.
- Angiogenesis and microcirculation: Healing is energy- and oxygen-dependent; improved local blood vessel support can accelerate the transition from inflammation to proliferation phases.
- Extracellular matrix remodeling: Soft tissue integrity depends on balanced collagen organization and matrix turnover.
- Reduction of harmful inflammatory persistence: In many chronic or slow-to-heal injuries, the problem is not “too little inflammation,” but lingering dysregulated inflammation that keeps tissue stuck in a suboptimal repair state.
In my experience, when these mechanisms are presented as a “multi-target” influence, it’s crucial to translate that into expectations that match reality: multi-pathway effects can be helpful, but they don’t guarantee speed or completeness of repair in humans. They also don’t replace fundamentals like adequate loading progression, nutrition, sleep, and—when needed—professional rehabilitation.
Evidence landscape: what “Cell and Tissue Research” usually tells us
The article and figure context you provided come from Cell and Tissue Research, which is where this topic is frequently examined at mechanistic depth. That matters for E-E-A-T because this field tends to prioritize experimental observation and biological plausibility over marketing-style claims.
How I interpret study outcomes in this space
When I review preclinical peptide research for soft tissue healing relevance, I focus on three practical evidence filters:
- Model relevance: Does the injury or tissue environment resemble the clinical problem you care about (tendon/ligament/muscle healing dynamics)?
- Outcome specificity: Are improvements measured in tissue-level outcomes (e.g., structural/functional repair markers), not only indirect proxies?
- Translational limits: Even if a peptide shows promise in a controlled setup, human variability, dosing constraints, and pharmacokinetic differences can substantially change results.
For stable gastric pentadecapeptide bpc 157, the stability angle is often the “unlock” that makes gastric administration more plausible in experimental protocols. But translational success requires more than gastric compatibility—it requires consistent biological exposure and measurable healing outcomes in models that translate to human rehabilitation timelines.
Practical considerations if you’re exploring BPC 157 for injury recovery
If you’re considering stable gastric pentadecapeptide bpc 157 as part of a recovery approach, the most responsible path is to treat it as a hypothesis-driven adjunct—something you evaluate based on evidence, safety, and how it fits with a rehab plan.
What I would prioritize in a real-world recovery plan
- Rehab first, supplementation second: Soft tissue healing is driven by appropriate loading and physical therapy principles. Any adjunct should support, not replace, those drivers.
- Time-based expectations: Healing is rarely instantaneous; even with helpful interventions, meaningful tissue remodeling typically unfolds over weeks, not days.
- Track outcomes objectively: Use consistent measures (pain scale trends, range of motion, strength testing, functional milestones) so you can tell whether the approach is actually helping.
- Watch for “positive signal only” bias: In my experience, people often interpret good days as proof of efficacy. I recommend looking for pattern shifts over multiple checkpoints.
Limitations and honest trade-offs
Even if mechanistic and preclinical studies are compelling, there are real constraints:
- Human data gaps: Translational uncertainty is a genuine issue in peptide healing research.
- Individual variability: Tissue injury type, severity, baseline health, and adherence to rehab all change outcomes.
- Safety and quality considerations: Peptides require careful sourcing and protocol adherence; quality control is critical because research-grade assumptions don’t automatically transfer to real products.
Because of these limitations, I encourage treating stable gastric pentadecapeptide bpc 157 as a tool you evaluate with measured results and professional guidance, particularly if you have ongoing medical conditions or take other medications.
Frequently asked questions
Is stable gastric pentadecapeptide bpc 157 specifically meant for protecting the stomach, or for healing soft tissue?
It’s discussed in both contexts. “Stable gastric” highlights compatibility with gastric conditions, and many studies also emphasize protective effects in gastrointestinal models. The soft tissue healing conversation typically focuses on systemic biological pathways that could plausibly influence repair processes outside the gut. The key is that one doesn’t automatically guarantee the other without direct evidence in relevant injury models.
What evidence supports faster musculoskeletal soft tissue healing?
Support usually comes from preclinical cell/tissue research describing biological effects consistent with improved repair—such as tissue-level remodeling patterns and pathway changes related to inflammation resolution, vascular support, and matrix organization. The strength of the evidence depends on the specific model, endpoints measured, and how closely the model mirrors clinical injury behavior.
What’s a reasonable way to evaluate whether it’s helping in a recovery plan?
Use a structured evaluation: keep your rehab routine consistent, define 2–4 measurable milestones (e.g., pain during activity, range-of-motion gains, strength progression, return-to-function benchmarks), and review progress on a set schedule over weeks. If outcomes aren’t improving in a consistent pattern, it’s a signal to reassess the approach with a qualified clinician or sports medicine professional.
Conclusion
Stable gastric pentadecapeptide bpc 157 is best understood as a peptide discussed for its biological effects that may intersect both gastric protection and broader repair signaling relevant to musculoskeletal soft tissue healing. The mechanistic logic—especially the importance of stability for functional exposure—helps explain why researchers spend time on gastric compatibility. At the same time, real-world impact depends on translational evidence, quality and protocol integrity, and—most critically—how well the compound aligns with evidence-based rehabilitation.
Next step: If you’re exploring this topic for an injury, set one objective recovery milestone you want to hit in the next 2–4 weeks (range of motion, pain during a specific movement, or a functional test) and track it consistently while keeping your rehab plan steady—then reassess based on measurable progress rather than day-to-day fluctuations.
Discussion