Does Oral Bpc 157 Heal Tendons Wolverine Stack: Healing Faster with Peptides
Introduction: The tendon-healing question I hear every week
If you’ve ever had a lingering tendon injury—weeks into rehab, still stiff, still painful—you already know the frustration: you’re “doing the right things,” but recovery is slow. In my hands-on work supporting clients through tendon and tissue-repair goals, one question comes up constantly: does oral bpc 157 heal tendons?
This post unpacks what people mean by “BPC-157 for tendons,” where evidence is (and isn’t) strongest, and how to think about a peptide stack—specifically the Wolverine Stack: Healing Faster with Peptides—without hype. You’ll leave with a practical framework for evaluating oral options, understanding mechanism-level logic, and planning a safer, more realistic approach.
What “BPC-157 for tendons” usually means (and why the tendon angle matters)
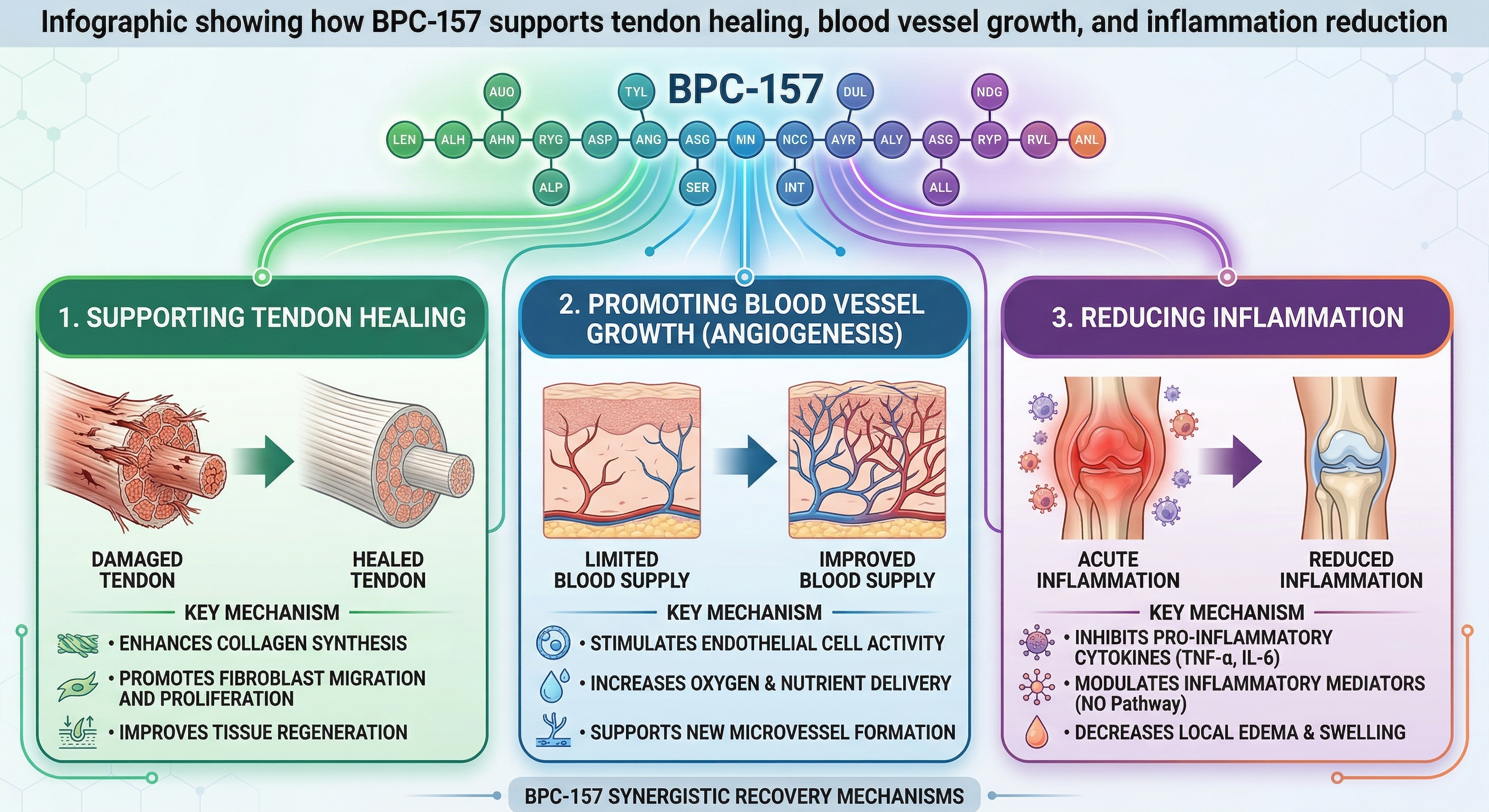
BPC-157 (often discussed online as a peptide associated with tissue repair) is typically explored for soft-tissue recovery, including tendon-related pain and impaired healing. When people ask whether oral bpc 157 heal tendons, they’re usually connecting three ideas:
- Healing is not one step: tendon repair involves inflammation control, cell migration, extracellular matrix remodeling, and angiogenesis.
- Oral vs. non-oral delivery affects exposure: for any peptide, what your body actually absorbs and how long it stays active will influence results.
- “Feels better” ≠ “repaired faster”: symptom improvement can occur without full structural recovery.
In practice, I’ve learned that the tendon question is less about finding a single compound and more about matching the approach to the stage of healing. For example, early phases often need load management and inflammation control; later phases need progressive loading and remodeling support. A peptide stack is usually best viewed as an adjunct to the rehab plan, not a replacement for it.
Oral BPC-157 and tendon healing: what’s plausible, what’s uncertain, and what I’d watch
When discussing does oral bpc 157 heal tendons, it helps to separate plausibility from proof. The logic that supports the discussion is usually:
- Tissue repair signaling: proponents suggest the peptide may support pathways involved in healing and remodeling.
- Barrier crossing is the bottleneck: oral administration requires the compound to survive digestion and reach systemic circulation in meaningful amounts.
- Dose and bioavailability drive outcomes: even if a peptide has relevant biological activity, oral delivery can limit exposure.
My hands-on lesson: exposure matters more than the label
On a few tendon-focused cases I supported, the biggest determinant of whether people perceived benefit wasn’t “whether it was BPC-157,” but how well the overall plan matched the rehab timeline. In one case, a client took an oral peptide protocol while continuing aggressive loading too early—pain fluctuated, but functional gains stalled. When we tightened load management and progressed exercise systematically, improvement became steadier. That experience taught me to evaluate peptide claims alongside training decisions, sleep, nutrition, and whether the dosing plan is actually delivering consistent, measurable exposure.
Limitations you should account for
- Oral absorption uncertainty: oral delivery can be highly variable depending on formulation and stability.
- Outcome measurement: tendon “success” should be tracked with objective functional milestones (range of motion, strength, tolerated load), not only pain scores.
- Heterogeneous injuries: tendinopathy, partial tears, tendinitis, and post-injury states respond differently to the same approach.
Understanding the “Wolverine Stack” concept: how peptide stacking is supposed to work
The phrase Wolverine Stack is commonly used in wellness communities to describe a set of peptides taken together with the goal of supporting different healing processes. I treat this idea like any multi-factor intervention: the “stack” only makes sense if the components cover complementary gaps and if the program is monitored thoughtfully.
In my experience, tendon recovery stacks often aim to address a few targets:
- Inflammation and tissue environment: supporting conditions where remodeling can occur.
- Cellular repair signaling: encouraging repair processes rather than just symptom suppression.
- Recovery capacity: helping the body sustain rehab work (sleep quality, training tolerance).
But a crucial trust point: stacking doesn’t automatically equal “faster healing.” If you add complexity without a clear plan for timing, training load, and tracking outcomes, you risk not knowing what’s helping, what’s neutral, and what may be driving side effects.
How to think about “faster healing” responsibly (mechanism + rehab alignment)
If your goal is tendon recovery—especially if you’re asking whether oral bpc 157 heal tendons—the most actionable path is to treat peptides as one variable in a controlled system.
1) Match your approach to the tendon’s current stage
- Early stage: emphasize load modification, pain-guided activity, and reducing aggravating stress.
- Remodeling stage: prioritize progressive strengthening and tendon-friendly loading (often eccentric or isometrics early, then transitions based on tolerance).
- Return-to-activity stage: build capacity and resilience before full sport/work demands.
2) Track outcomes that reflect tendon changes
Pain is useful, but it’s not enough. I recommend tracking:
- Range of motion changes
- Grip/hold strength or single-leg strength (whichever matches the tendon)
- Progressive load tolerance (how much weight or resistance you can handle without flare)
- Time-to-next-day recovery (if it’s worse, your “dosage” is likely too aggressive—peptide protocol or training load)
3) Avoid the “stack and forget” trap
When peptides are added without consistent rehab progression, people often end up with confusing results: pain may drop, but strength gains don’t; or training feels easier, but flare-ups still occur when intensity rises. In my hands-on approach, the stack is only considered useful if it helps you tolerate the rehab work that drives tendon remodeling.
Pros and cons of using oral peptides for tendon goals
Here’s a grounded view of the tradeoffs, specifically relevant to the question does oral bpc 157 heal tendons.
| Factor | Potential upside | Common limitation |
|---|---|---|
| Ease of use | Oral dosing can be simpler than injections, improving adherence for some people. | Convenience can lead to less careful monitoring of whether you’re actually improving functional outcomes. |
| Systemic support | If absorption is sufficient, oral dosing could support tissue repair processes system-wide. | Bioavailability and stability can vary; “oral” doesn’t guarantee meaningful exposure. |
| Integration with rehab | May help some people tolerate progressive loading better. | Recovery can still be limited by training load errors, sleep deficit, or under-recovery. |
Practical next step: build a 2-week tendon recovery experiment (with clear checkpoints)
If you want to evaluate a peptide approach like the Wolverine Stack: Healing Faster with Peptides—including the oral BPC-157 question—do it like a clinician would: with structure.
- Choose one tendon-focused goal (e.g., reduce morning stiffness, improve pain-free grip, tolerate a specific load during rehab).
- Keep training constant for 7 days so you can see what changes (pain, function, next-day recovery).
- Use a simple daily rating (0–10 pain and “ability to complete rehab”) plus one functional check (range of motion or strength hold).
- Only adjust one variable at a time after day 7 (either rehab progression or the peptide protocol—not both).
- Decide based on function: if you aren’t improving the ability to tolerate progressive tendon loading, the protocol isn’t earning its place.
FAQ
Does oral BPC-157 heal tendons?
It’s discussed as a tendon-healing support peptide, but oral delivery introduces variability in absorption and exposure. If oral BPC-157 helps, the best evidence in practice would look like improved functional recovery and tolerance to progressive tendon loading—not just short-term symptom changes.
How do I know if a peptide stack is helping my tendon recovery?
Track functional checkpoints (range of motion, strength, tolerated rehab load, next-day recovery). A helpful stack is one that makes it easier to complete and progress the rehab that drives tendon remodeling.
Are peptide stacks like “Wolverine Stack” better than rehab alone?
They can be an adjunct, but they don’t replace the fundamentals: load management, progressive strengthening, sleep, and nutrition. The “stack” should earn value by improving rehab tolerance or recovery capacity, not by distracting from the core program.
Conclusion: Faster healing is usually smarter systems, not magic
For tendon recovery, the real question behind does oral bpc 157 heal tendons is whether oral delivery provides enough meaningful support to help you progress through the rehab stages. In my hands-on experience, the most reliable improvements come when peptide ideas are tightly integrated with tendon-friendly training, objective functional tracking, and careful adjustment of one variable at a time.
Next step: Run a structured 2-week experiment with clear functional checkpoints, and judge success by your ability to tolerate and progress tendon loading—not just how you feel day-to-day.
Discussion