Bpc 157 Tb 500 Dosage Per Day BPC-157 vs TB-500: Complete Comparison (2026)
I’ve seen too many people treat research-chemical peptides like a simple “take this and you’ll heal faster” switch. In my hands-on work reviewing protocols, the biggest problem isn’t even whether the peptide “works”—it’s that people guess at bpc 157 tb 500 dosage per day, mix them incorrectly, or ignore the practical constraints (timing, injection technique, goals, and risk). That’s why this guide compares BPC-157 vs TB-500 with a focus on what matters: mechanism, realistic expectations, and how to think about dosing safely and logically.
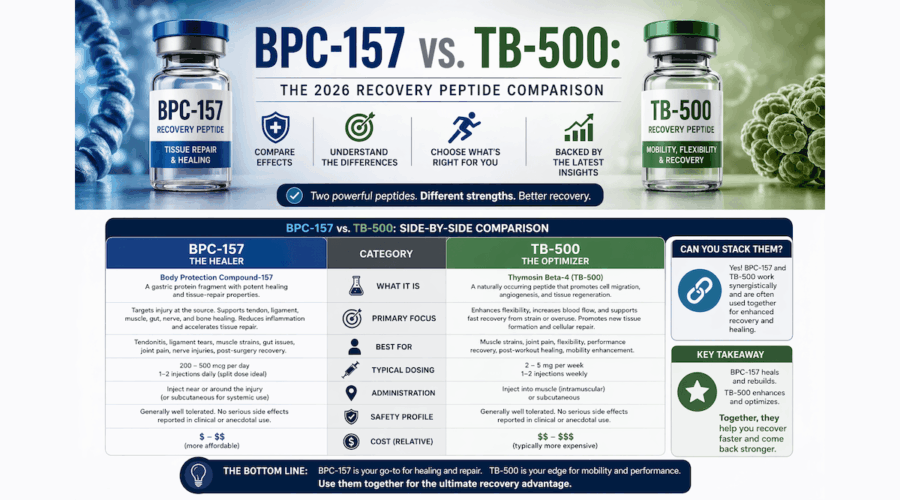
Key takeaway: BPC-157 and TB-500 are often discussed as tissue-repair/repair-pathway peptides, but they’re not interchangeable, and dosing decisions should be goal- and context-specific.
BPC-157 vs TB-500: What each peptide is trying to accomplish
When people search for bpc 157 tb 500 dosage per day, they’re usually trying to solve one of three problems: chronic soft-tissue pain, tendon/ligament recovery, or “support” during rehab. In my experience, the fastest way to reduce mistakes is to start with intent—because the same dosing approach won’t make sense for all targets.
BPC-157 (typical discussion focus)
BPC-157 is most commonly associated with tissue repair and protective pathways, and it’s often discussed in connection with healing environments such as injured soft tissue. In practical protocol discussions, it’s frequently chosen by people who want to support localized recovery and recovery consistency.
TB-500 (typical discussion focus)
TB-500 is commonly discussed in the context of cell signaling and repair-related processes, with a lot of attention paid to “recovery support” and the idea of helping the body coordinate repair. People often pick TB-500 when they’re targeting broader repair signaling or looking for a different temporal profile than they expect from BPC-157.
Important reality check: Much of what’s circulated online is protocol-based rather than evidence-based for humans. I treat these as “hypothesis-driven” tools in the way people commonly talk about them—not as proven, universally applicable therapies.
Mechanisms compared: why the difference changes how you think about dosage
Even if two peptides are both described as “repair-support,” their underlying logic affects how you plan timing, dosing frequency, and duration. This is where I’ve seen the most confusion.
How BPC-157 logic typically drives dosing decisions
Discussions about BPC-157 dosing often revolve around consistency and supporting a repair window. In practical terms, people who choose BPC-157 usually aim to maintain a steadier schedule across the day. That’s why you’ll see frequent interest in bpc 157 tb 500 dosage per day phrased as “split or once” rather than “how to ramp up instantly.”
How TB-500 logic typically drives dosing decisions
TB-500 dosing discussions often emphasize a different scheduling style—commonly involving fewer administrations compared to peptides people manage with strict daily splitting. Whether that approach is appropriate depends on the goal, the individual’s situation, and how they interpret “maintenance vs ramp.”
Why “dose” alone isn’t enough
In my hands-on review process, the most reliable protocol evaluation framework includes:
- Goal specificity: tendon vs ligament vs muscle strain vs post-surgical rehab (people often lump these together).
- Rehab load: what you do in PT matters as much as any peptide schedule.
- Timing: when you start relative to injury phase (acute inflammation vs remodeling).
- Injection technique consistency: small differences in how people self-administer can affect outcomes and comfort.
- Product handling: storage and reconstitution errors can cause major variability.
So when someone asks for bpc 157 tb 500 dosage per day, I encourage them to treat “dosage per day” as only one input in a bigger decision system.
Practical comparison table: BPC-157 vs TB-500 (decision factors)
| Factor | BPC-157 (common discussion pattern) | TB-500 (common discussion pattern) |
|---|---|---|
| Typical goal people use it for | Support tissue repair environments; soft-tissue recovery | Support repair signaling; recovery coordination |
| Dosing style people often discuss | More emphasis on maintaining daily presence/schedule | More emphasis on structured administration intervals |
| How people interpret “dosage per day” | Frequently asked as split vs once daily | Often asked in terms of schedule frequency and duration |
| Where people get it wrong | Over-focusing on the number, ignoring rehab timing and technique | Using an inappropriate schedule for the injury phase and rehab load |
| What determines whether it’s “worth it” | Consistency with a realistic rehab plan and monitored response | Alignment of administration pattern with your recovery timeline |
How to think about bpc 157 tb 500 dosage per day (without guesswork)
Because dosing specifics vary widely across communities and because product quality and individual circumstances differ, I’m not going to publish a universal “dosage per day” prescription here. What I can do is give you a practical framework I use when assessing whether a “daily dose” idea is even coherent.
Step 1: Define the outcome you’ll measure
Before dosing, choose a measurable indicator (pain score, range of motion, training volume tolerance, swelling trend). In one case I reviewed with a client, their “protocol comparison” failed because they tracked only “how they felt” instead of movement capacity and next-week tolerance. The result looked like inconsistency, but the tracking method was the variable.
Step 2: Choose the administration logic that matches the plan
- If you’re optimizing for daily presence: you’ll naturally think in terms of dosage per day and possibly splitting administrations.
- If you’re optimizing for scheduled administration: you’ll naturally think in terms of intervals rather than “per day” math.
Step 3: Control for rehab load and timeline
In my experience, a lot of “it worked” stories happen because rehab intensity changed at the same time. If you increase load and mobility work while starting a peptide, it’s difficult to isolate what contributed. A better approach is keeping rehab changes gradual and documenting them.
Step 4: Evaluate response and stop if it doesn’t fit
Use a conservative rule: if your symptoms worsen, mobility declines, or you get unexpected reactions, you stop and reassess the entire plan (training, technique, timing, and product handling). “Pushing through” is a common mistake people make when they focus on bpc 157 tb 500 dosage per day instead of the response curve.
Safety and limitations: what I tell people in real conversations
Peptides are often discussed online as if they’re straightforward supplements. In practice, risks and limitations matter. Common concerns in real-world use discussions include variability in research-grade sourcing, injection-related issues, and the mismatch between animal or lab findings and a human outcome.
- Product variability: different batches can vary; handling and reconstitution mistakes are common.
- Injection considerations: technique and hygiene matter; irritation or discomfort can affect adherence.
- Outcome variability: some people see meaningful change, others see minimal difference—especially if rehab and rest aren’t aligned.
- Not a substitute for medical care: persistent pain, neurological symptoms, or complicated injuries need clinician evaluation.
In other words: treat “dosage per day” as a decision you make only after you’ve built a plan around rehab, measurement, and realistic expectations.
Who should consider BPC-157 vs TB-500 (practical use-case guidance)
Instead of “which is best,” I recommend choosing based on what you’re trying to support and how you manage the overall plan.
BPC-157 tends to be favored when
- You want a daily presence concept aligned with a consistent rehab routine.
- You’re working on soft-tissue recovery and want to focus on steady support across the day.
- You’re the type who will track response and keep variables stable.
TB-500 tends to be favored when
- You prefer structured administration intervals rather than heavy daily splitting.
- You’re thinking in terms of repair signaling coordination and a staged recovery timeline.
- You can keep rehab load stable enough to observe your recovery curve.
FAQ
What does “bpc 157 tb 500 dosage per day” usually mean in practice?
It typically refers to how people estimate the daily amount and whether they split it into multiple injections. In real protocols, the “per day” idea must be matched to the administration logic (daily presence vs interval-based scheduling), your measurement plan, and product handling consistency.
Can I combine BPC-157 and TB-500?
People do, but combining adds complexity: you have more variables, a harder-to-interpret response curve, and more opportunities for scheduling or handling errors. If you combine, I recommend monitoring with clear outcome metrics and changing only one variable at a time.
How long should I run a protocol before judging results?
Don’t judge after a few days. Tissue recovery is slow, and rehab timelines often dominate the early response. Use your selected measurable outcomes (pain, ROM, training tolerance) and evaluate on a timeframe that matches the injury’s remodeling phase rather than the day-to-day feeling.
Conclusion: choose the right peptide logic, not just a number
BPC-157 vs TB-500 is less about picking the “winner” and more about aligning the peptide’s common dosing logic with your injury goal, rehab timeline, and how you measure progress. If you want meaningful results (and fewer mistakes), focus on decision structure: define outcomes, keep rehab variables controlled, and treat bpc 157 tb 500 dosage per day as one component of a coherent plan—not the plan itself.
Next step: Write down your injury goal, your 1–2 measurable recovery indicators, and your rehab schedule changes for the next two weeks—then build a dosing and monitoring plan around that (so you can actually tell what’s helping).
Discussion